The World Health
Organization (WHO) was notified of the first cases of Ebola in Guinea, West
Africa in March 2014. Since then, the virus has spread past Guinea, thanks to
the region’s porous borders, into Sierra Leone, Liberia, Senegal, and Nigeria.
With a fatality rate of 70%, slightly lower than the 90% fatality rate of past
outbreaks, Ebola has had a chance, due to unprepared public health systems and
poorly informed citizenry, to spread steadily through the region. Ebola is
thought to have spread to humans through fruit bats, which are considered a
delicacy for some West Africans, as well as through other types of bush meat such
as small rodents.

While Ebola does not
spread quite as quickly as the Spanish flu or pre-vaccination days measles,
efforts to contain the disease have already exceeded the capacity of public
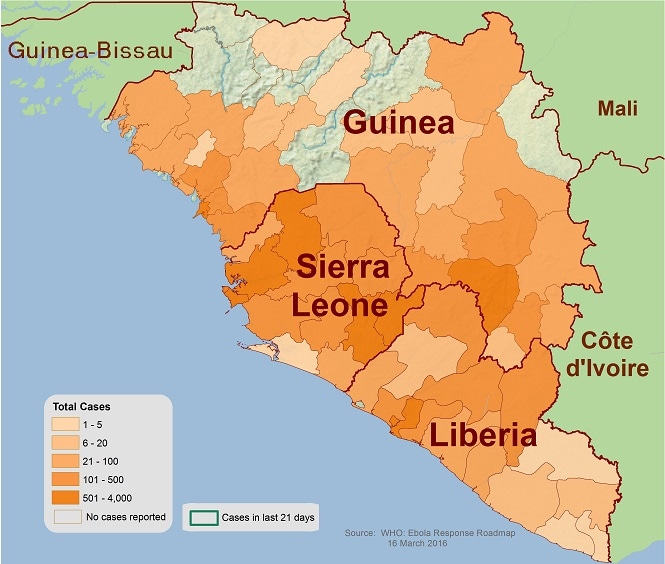
health systems in West Africa. The total case count of the disease has reached
6,574, as of September 29th, according to the US Centers for Disease Control
and Prevention (CDC). According
to the CDC, the total number of laboratory confirmed cases is 3,626 and the
total number of deaths is 3,091. The overwhelming majority of these cases have
been documented in Liberia (3,458 total cases, 914 laboratory confirmed cases,
and 1,830 deaths), with Sierra Leone running a close second (2,021 total cases,
1,816 laboratory confirmed cases, and 605 deaths). In Senegal, no new cases
have been reported since August 29, and in Nigeria, no new cases have been
reported since September 5. In Guinea, the infection rate seems to have
stabilized.
How many people are or will be affected?
Gaining an
accurate total of the number of Ebola cases has been complicated by several factors, the first being simply that
many cases of Ebola are going unreported. The CDC estimates that for each
reported case of Ebola, another 1.5 cases are not documented. Part of this is
caused by understaffed clinics and hospitals that lack the resources to admit
and treat everyone who shows up, leading to an incomplete total count of
afflicted persons. A failure to self-report further compounds the problem. In
many communities, there is a stigma attached to Ebola, and people are unwilling
to admit that someone in their family or household is showing symptoms of or
has Ebola. The threat of quarantine or restrictions on freedom of movement also
make it less likely that people will self-report, further hindering efforts to
stamp out the disease.
Creating a
predictive model to project the potential impacts of Ebola before the epidemic
ends has also proven difficult. The CDC is working with data being reported
from disconnected streams, which increases the possibility for duplicate
reports of the same cases. Differences in reporting reliability and variations
in levels of underreporting make it difficult to apply accurately one
predictive model across all of West Africa.
The efforts to
combat and contain the spread of Ebola have been hampered not only by a lack of
resources available to the local governments and medical centers, but also by
the general distrust that Western medical response teams have encountered.
Rumors that Ebola is a conspiracy by the Americans or the Western world to kill
the locals have led to tense relationships between local communities and aid
workers, escalating in one publicized instance to the incident in Guinea this
past month in which the members of a health delegation were actively targeted
and killed by the local community. Such beliefs also dampen the likelihood that
people will seek professional medical attention or follow proper sanitation
protocols if and when they begin to show symptoms, thus increasing the risk to
their family members, close friends, and untold others.
Local Efforts and Challenges
In Liberia, Médecins
Sans Frontières (MSF) is attempting to double current capacity to 400 beds at
its facility in the capital city of Monrovia by the end of the month. To ensure
adequate treatment, the facility is increasing staff as well. MSF’s Monrovia facility
currently has 617 health care workers for the 200 beds. However, death toll for
Ebola victims is rising rapidly in Liberia mostly due to the lack of access to
medical care. Most infected people are treated in their homes by family members
who then contract the disease. Even when ambulances and response teams make it
to the countryside, they do not have the capacity to transport all of the
infected people back to a hospital or mobile clinic. They also face resistance
from people who are afraid to leave their families to go, very likely, to their
deaths in a cold hospital room surrounded by foreign health workers covered
head-to-toe in protective gear. The country does not have the resources to
force infected or potentially infected persons into treatment in isolation
units in hospitals.
In Sierra Leone,
where about 600 people have died of Ebola, a quarantine and curfew have been
imposed on five of the 13 counties, affecting mobility for a third of the
country’s 6 million citizens. Quarantine has led to riots and frustration as
people are disappointed with the lack of progress in ridding the country of
this disease. Further frustrating efforts to combat the spread of the disease,
funeral customs and traditions in the region run counter to the safe burial and
disposal protocols necessary to prevent infection.
US Efforts
Local
governments in West Africa unfortunately lack the capacity to combat this
epidemic on their own. The US has taken the lead in a four-pronged effort, with
the support of the international community. The strategy commits the expertise
of the US military to coordinate and facilitate international relief efforts by
expediting the transportation of supplies, medical equipment and personnel, to
build Ebola Treatment Units in hard hit areas, to set up facilities to train an
additional 500 medical staff per week. USAID, along with other US Government
agencies, is spearheading efforts to disseminate awareness and protection kits
primarily in Liberia, as well as across the region. Complete details on the US
strategy can be found here.
The Pentagon
announced yesterday that it would be bolstering its existing efforts to combat
Ebola in West Africa by deploying the 101st Airborne
Division. The 1,600 US troops will be assisting in coordinating the global
response to the Ebola epidemic. In addition to these troops who will be trained
on the particulars of the disease and personal protective equipment, there is
also a team of 700 engineering troops en route to the region tasked with the
building treatment centers desperately needed to treat infected people. These
engineers will be joining the US Navy’s construction arm, which began assisting
crews in Monrovia, Liberia last week in the development of treatment and
training centers.
International Efforts
With infection
numbers surpassing 6,500 by the end of last month, and reported numbers
estimated to be about half or ⅓ of total infections, the international
community has been quick to make promises of much needed aid. Making good on
those promises with efficiency will be imperative to the success of containment
efforts. This past week, UN Secretary General Ban Ki-moon set up the UN Mission
on Ebola Emergency Response, and the UN opened up a regional headquarter in
Accra, Ghana to assist regional efforts in affected countries.
Global health
experts estimate that in order to make real progress on stemming the tide of
Ebola in the next two months, at least 70% of those infected should be
receiving treatment and 70% of burials should follow safety protocols. This
ambitious goal will require significant assistance from the international
community in terms of money, infrastructure and health personnel. The 800
additional beds promised by the international community fall woefully short of
the 3,000 beds estimated by the WHO as needed to meet current demands. Cuba has
sent 461 doctors and nurses, China has sent a 59-person team and a mobile lab
to Sierra Leone, and Britain has promised facilities for 700 new beds.
Economic Impact
The Ebola
epidemic certainly poses a genuine threat to international public health and
security, which has galvanized the international community into acting, but the
epidemic has already devastated the economies of the hardest hit countries.
Though Guinea has been able to stabilize Ebola infection rates, the country is
facing significant economic losses. $30 billion worth of infrastructure and
mining construction have come to a halt, and the country faces a loss of up to
2.5 percentage points of estimated GDP growth. Multiple industries have been
impacted in Liberia by decreased worker mobility due to internal travel and
public transport restrictions: fuel sales have dropped 20 to 35%, and rubber
and palm oil production and distribution have been disrupted. Misconceptions
about Ebola transmission has fueled beliefs that the disease can spread through
crops, water or food, leading to communities abandoning agricultural
production, which is only compounding existing food shortages from
transportation disruptions.
What’s Next?
The reach and
intensity of this Ebola epidemic remains to be seen, but efforts to contain and
quash the disease are likely to ramp up as the CDC confirmed yesterday the
first ever case of Ebola diagnosed on US soil. The patient, a man who traveled
from Liberia to Dallas, is in serious condition and is being treated in
isolation at Texas Health Presbyterian Hospital. Some people who came into
contact with the man after he became symptomatic, including school-age
children, are being monitored for symptoms as well, while a CDC team has been
dispatched to Dallas to investigate and monitor for 21 days any other persons who
might have come into contact with the patient.
The hysteria has
already begun to spread in light of the Texas diagnosis, with Americans
unnecessarily panicking that there will be an Ebola epidemic in the US.
Hopefully, this incident will increase pressure on the pharmaceutical companies
currently testing and producing the Ebola vaccine. The CDC has increased
ongoing efforts to raise awareness about affected countries, important travel
precautions, and the symptoms and transmission of the disease. Ebola doesn’t
spread until a person is symptomatic, therefore proper steps should be taken to
investigate travel histories of all those entering the US in order to monitor
those who have traveled to West Africa. If medical teams are able to isolate
and treat those who show the slightest symptoms, as well as any persons who
have had recent contact with the infected person, there shouldn’t be an Ebola
epidemic in the US.
As for West
Africa, let’s hope the international community musters up the resources and efficiency
needed to contain the disease before too many more people die.
No comments:
Post a Comment